A Testing Time Part 3 – Hormone Pregnancy Tests
by Margaret Sparrow
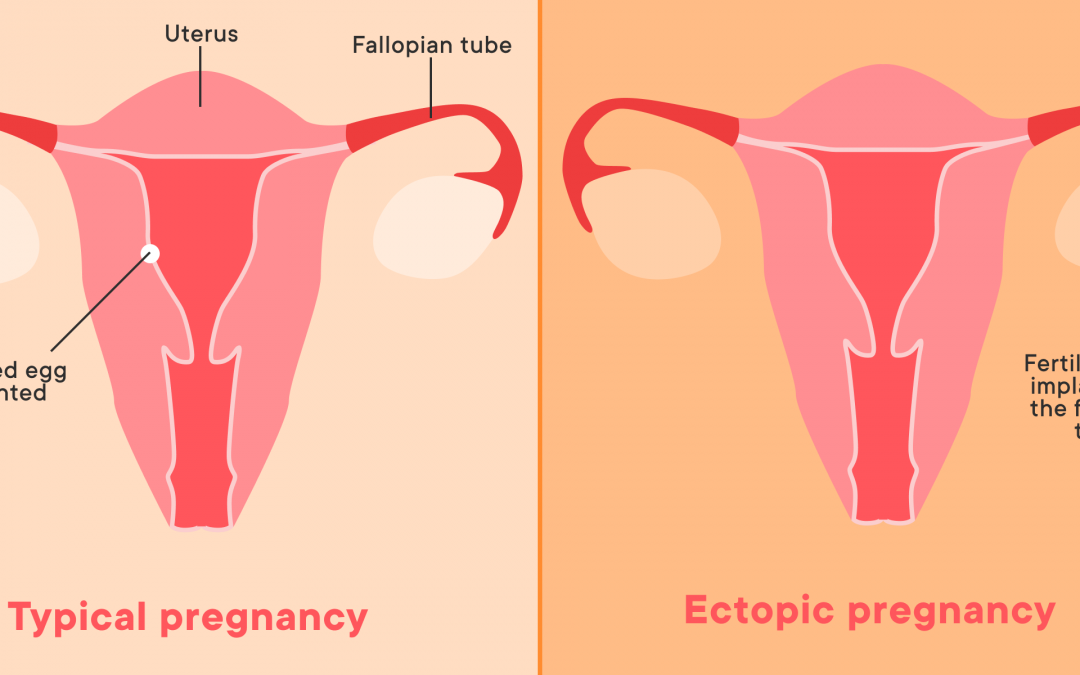
From 1942 another type of pregnancy test was developed, not using hCG but two other hormones, oestrogen (or a synthetic oestrogen) and progesterone (or a synthetic progestogen). Either taken orally or injected, various combinations of these hormones induce menstruation but only if the woman is not pregnant or possibly if the pregnancy is not well established. There is limited evidence that it was used to induce an abortion. No bleeding is a positive pregnancy test.
Two brands of Hormone Pregnancy Tests (HPTs) were available in New Zealand – Primodos by Schering from 1966 to 1975 and Amenorone Forte by Roussel from 1968 to 1975. Both were composed of the same hormones found in some contraceptive pills but the progestogen was in a much higher dose. It is not known to what extent these tests were used in NZ. The alternative, used by most doctors at that time, was to send a morning urine sample to the laboratory for one of the hCG tests, 14 days after the missed period.
Because of the reported risk from overseas of congenital malformations associated with the administration of these hormones during early pregnancy, both HPTs were withdrawn by the NZ Department of Health in 1975. Forty-seven years later, on 20 March 2017 the NZ Ministry of Health, responded to renewed concerns locally and in the UK and issued a statement confirming that Primodos had been used in NZ but that no fetal abnormalities had been notified to the NZ Centre for Adverse Reactions Monitoring (CARM). As a result of the publicity 10 historic cases were notified to CARM as possible adverse reactions but with the time lag it would be impossible to prove causation. The Ministry stated it would liaise with the British equivalent of CARM, the Medicines and Healthcare products Regulatory Agency (MHRA) for further developments.
The result, silence.
So what was the Primodos story in the UK?
1958
Primodos was introduced in Britain and was supplied on prescription for 20 years until 1978.
1967
Paediatrician Dr Isabel Gal published the first comprehensive study identifying an association between HPTs and congenital abnormalities. Dr William Inman Principal Medical Officer of the Medicine Control Agency was dismissive of her findings despite the fact that HPTs were introduced at about the same time as Thalidomide which also caused congenital abnormalities.
During the next 8 years Inman conducted his own study and during that time confidentially warned the German manufacturer, Schering, of possible legal consequences, but did not raise the issue with the public as might have been expected. Some commentators suggest that one factor may have been that these were the same hormones that were used in the contraceptive pill and publicity would have created a pill scare.
1975
Dr Inman published an interim report and the first public warning was announced regarding Primodos. This was heeded in NZ but not in the UK although a warning appeared on the packet.
1977
A second warning to doctors stated “The association has been confirmed.” Archival documents reveal that at this time the probability of birth defects after taking Primodos was estimated to be 1 in 5. Inman’s evidence was destroyed eliminating its use in future case investigations.
1978
Primodos withdrawn in the UK.
The Association for Children Damaged by Hormone Pregnancy Tests (ACDHPT) was formed to advocate for some 800 affected families.
1982
ACDHPT, using legal aid, prepared to take a case to court but a causal link was too difficult to prove and the case was too costly to pursue. Inman gave evidence for Schering.
2006
Schering was sold to Bayer who then became responsible for any litigation.
2014
MHRA published an assessment of historical evidence on Primodos and congenital malformations and found the results inconclusive.
2017
An Expert Working Group commissioned by the UK Government concluded there was no association. In the opinion of ACDHPT this was a whitewash and PM Theresa May responded to the clamour by commissioning an independent review, not only of Primodos but also the use of sodium valproate (a drug for epilepsy) in pregnancy and vaginal mesh.
2020
“First Do No Harm” The report of the Independent Medicines and Medical Devices Safety Review, chaired by Baroness Cumberlege, concluded that there was an association between Primodos and adverse effects and that Primodos should have been withdrawn in 1967, immediately after the publication of Dr. Gal’s Study. Recommendations were made to improve safety in the future. And so the campaign continues…
For further information see the website of ACDHPT
Dame Margaret Sparrow was a medical doctor, abortion provider, and president of ALRANZ for many years.